
Table of Contents
Are non-English-speaking clients found as immediately in the unexpected emergency section (ED) as English-talking people? If not, is this gap restricted to selected non-English languages, or is it steady across all non-English languages? Is this gap dependable on weekdays? Is it far more pronounced on weekends?
It would be almost unachievable for a medical or economical functions group in your typical emergency department (ED) to solution these questions promptly and precisely with no the appropriate details. What is much more, except an personal has an analytical history, it would be very tough for them to know the place to start with information exploration. But these forms of thoughts are critically vital and relevant to being familiar with wellness disparities and in the end, wellbeing equity.
The COVID-19 pandemic surfaced longstanding social and racial inequities, and COVID’s disproportionate influence on folks from some racial and ethnic teams offered a obvious instance of enduring health disparities across the country. Attempts at the federal, condition and local levels are very well underway to begin to mitigate these disparities, which includes increasing knowledge transparency and improving the equity of care shipped through the overall health treatment continuum.
A single instance of this sort of an effort and hard work is at the Section of Crisis Medication at the University of Michigan Health-related Faculty, in which Dr. Christopher Fung, MD, led the growth of an EHR-derived overall health fairness dashboard to allow for for the exploration of disparities in ED treatment. We not long ago spoke with Dr. Fung about the dashboard and how enhanced obtain to data and metrics enables exploration and identification of wellbeing disparities that may well need more investigation.
Responses have been edited for clarity.
Can you explain the intervention to produce a dashboard on disparities in the ED?
As an analytics particular person, I care about gathering the ideal information in order to make information-knowledgeable decisions. So generally, creating a data dashboard like this is helpful for two things: approach monitoring and information exploration. With system monitoring, we’re speaking about monitoring a distinct course of action above time utilizing a metric you know extremely effectively (i.e. the amount of clients viewed per hour) whereas details exploration is extra about asking inquiries of details, commonly with a speculation by now partially shaped or personal observations that you’d like to check out even further. For case in point, you could question if there are differences in how swiftly suffering medications are supplied to individuals of a unique race, or distinctions in the time it normally takes to see a medical professional relying on your race. Without having a thing like a dashboard that enables you to slice and dice knowledge, it is quite challenging to investigate these wellness disparities to appropriately obstacle a hypothesis. For this project in individual, we leaned extra in the direction of the data exploration facet of items but the dashboard is undoubtedly valuable for approach monitoring way too.
The edge of working with ED data, as opposed to other pieces of the hospital other than most likely the operating place (OR), is that all of our metrics are typical and very well-validated since in the end, EDs want to be as economical as feasible. Most EDs in the place are presently meticulously monitoring points like waiting place time, how prolonged it will take for the doctor to see a affected individual, how very long it takes to get agony drugs and how lots of CT scans or X-rays are ordered. However, it is exceptional that this knowledge is stratified by teams that have the opportunity to be marginalized in their care for case in point, race, ethnicity, sexual orientation, gender id, language, faith, age, and bodyweight, among other folks. Moreover, it is scarce that this sort of data is available to individuals outdoors clinical and economic functions, this sort of as resident doctors or other trainees.
What led you to take on this effort and hard work? What position did resident physicians engage in in this task and how has it been practical for them?
Our objective with this venture was to build a data dashboard that would deliver resident physicians with all set obtain to ED information to facilitate exploratory assessment on disparities in ED affected individual treatment as part of an current high quality improvement (QI) method. Resident doctors in EDs across the country enjoy a essential purpose in client treatment nevertheless numerous of them have limited obtain to related details and restricted chances to engage in eliminating health and fitness treatment disparities. Not only is the necessary knowledge ordinarily not obtainable to residents, but it is also challenging for them to recognize and interact with the facts to get the results they are just after.
The EHR-derived health equity dashboard, which went reside in September 2021, is specially beneficial for residents as they do the job on the QI assignments they are tasked with to enhance overall health fairness concerns. The dashboard supplies a one of a kind viewpoint enabling citizens to visualize information nevertheless they want to uncover or check out disparities, start out to understand root results in, establish interventions and measure their impression.
Our first eyesight was that anyone in the ED would have entry to this dashboard and in specific, resident medical professionals could work with their mentors on QI projects. The truth is that residents are unbelievably occupied a lot of of them operate 60-80 several hours and even though some are very study-pushed and have interacted with the dashboard, the uptake has been slower than we anticipated. That stated, we just rolled this out in September 2021 and new procedures and workflows get time to rollout so we’ll see what the utilization seems like as we go ahead.
How is the dashboard being utilised by medical personnel?
A ton of people are working with the dashboard but there are a lot of state-of-the-art sights and buttons, which can be a small frustrating. There is a variation concerning a thing published for mass usage, like what you could obtain on The New York Times’ “The Upshot” or FiveThirtyEight, the place it is more details-driven journalism with a simple visualization, than a strong data dashboard like ours. As you get started incorporating interactivity to a dashboard, it can grow to be additional and more too much to handle with each individual button you can click on or choice you can transform. So that’s a problem for us to get over finding people of the dashboard to interact with it but not in a way which is frustrating to them or confuses the photo far more.
My basic feeling is that men and women are considerably more ready to acknowledge knowledge journalism than they were just a several many years ago every single media organization is executing that now. The typical general public is having much more snug with information currently being introduced this way and the exact issue is happening in wellbeing treatment with these kinds of dashboards and details visualizations.
What classes have you uncovered since employing? Did you explore one thing unanticipated?
Further than the usability obstacle I explained, I did not know how challenging it was for management to get information out of the Byzantine process that is an digital medical report. Because placing the dashboard out there, I’ve quickly understood how earlier inaccessible this info was. Ahead of I designed the dashboard, the old way to get that knowledge was to send a bunch of email messages that ultimately finished up with an analyst managing static studies. Now, it’s significantly a lot easier to ship somebody a link to the dashboard and they can look at for by themselves.
On the other hand, it receives a very little little bit into the weeds when you insert state-of-the-art features like comparing two groups towards every other for some metric that can develop into a minor mind-boggling to folks. So which is sort of my ‘side job’ as a information scientist building the dashboard a lot more usable for men and women other than just myself.
What are your future options for the dashboard? What updates have you produced to the dashboard? What is the standing of some of the ‘future directions’ mentioned in the research?
My main task for this line of investigation is making use of facts to drive some of our DEI and fairness initiatives. Specifically, encouraging extra use of the dashboard amongst the trainees – both equally resident physicians and learners. They are often tasked with coming up with well being treatment equity QI tasks and there is a wealth of facts they can use to justify the venture they are performing which is essential simply because most assignments involve invest in-in from nursing staff, administrative team, and so on. Initiatives also necessitates funds, so it is vital to back up QI project requests with challenging details. I want to make the trainees’ interactions with the dashboard – and info in general – smooth plenty of so that a person without having an analytical history can do it. They need to be in a position to build the query and then go to the knowledge for a much more in-depth examination to develop a rationale for their QI initiatives, or to arrive up with new QI projects.
In terms of foreseeable future instructions, fairly much each ED in the region has this sort of information already these information sets we’re employing are not that unusual. They are all live and they are all all set for analytics they just require to be overlaid with some things that may add to wellbeing care inequalities like age, race, gender, and many others. So the for a longer period term energy is to scale you can scale across a greater health care program or even unrelated EDs mainly because anyone has this information currently you just require the platform to put it together in a dashboard.
What other wellness fairness operate are you enterprise or preparing to undertake? How can wellness IT gasoline individuals efforts?
A person of the factors I’m fascinated in discovering is how the triage approach biases treatment in the ED. Most individuals do not comprehend how influential people notes are they closely affect how immediately you are seen by a doctor. In many cases that piece of documentation is the only piece that is concluded in your initial working day at the medical center, so absolutely everyone is looking through this a single triage take note when you are in the ED. If that take note has inaccurate facts or it is biased, that influences your care. For case in point, if you exhibit up at the ED in agony but you seem wonderful, the be aware will mirror that and there could be an assumption that you never require to be found as urgently. Correct or erroneous, those statements or notes are biasing and they impact far more than just time they also influence whether or not you get suffering prescription drugs, get a CT scan, and so on. So the language that we use in these notes is probably biasing and which is where by I’m starting a new line of study dissecting the language we use in triage notes and how that influences treatment down the street. It is very likely we are biasing treatment throughout language or race even if that is not at all our intention for case in point, physicians are inclined to describe women as “hysterical” and that has a biasing result on what providers believe of that patient, right before they even go in the room and meet the affected individual. An additional component is designing interventions to decrease that.
The function a dashboard could perform in something like that is operating an algorithm that analyzes the text of the notes primarily based on a language disparity rating, to identify irrespective of whether or not that language could result in disparities in care. One thing like this would be beneficial to nurses, vendors and other people so they can improved recognize how the language in notes can be biasing and in the long run, attract a clearer line in between language and outcomes.
What’s one thing that we did not deal with about this undertaking that we need to have?
We have collected a great deal of information and facts and have a dashboard but some thing that’s not highlighted in the article is truly the subsequent move with a challenge like this is having leadership purchase-in. In the end, it’s genuinely tough for any project to obtain momentum with no leadership fascination. I’m a school member at a large educational healthcare facility with accessibility to all sorts of resources and persons who can assistance me do items even then it is quite, really challenging to change a huge ship except the captain of the ship is acquired in to where you want to go.
To master additional about ONC’s get the job done to embrace wellbeing equity by structure, stop by HealthIT.gov. To find out far more about the College of Michigan’s overall health equity dashboard, study the study.

Figure C: Time to first suffering treatment by race. Most typically administered ache remedies had been discovered a precedence. Documented administration time is plotted as a survival curve the place administration of ache medication is the event of desire. Reduce curves show bigger chance of receiving pain medication.
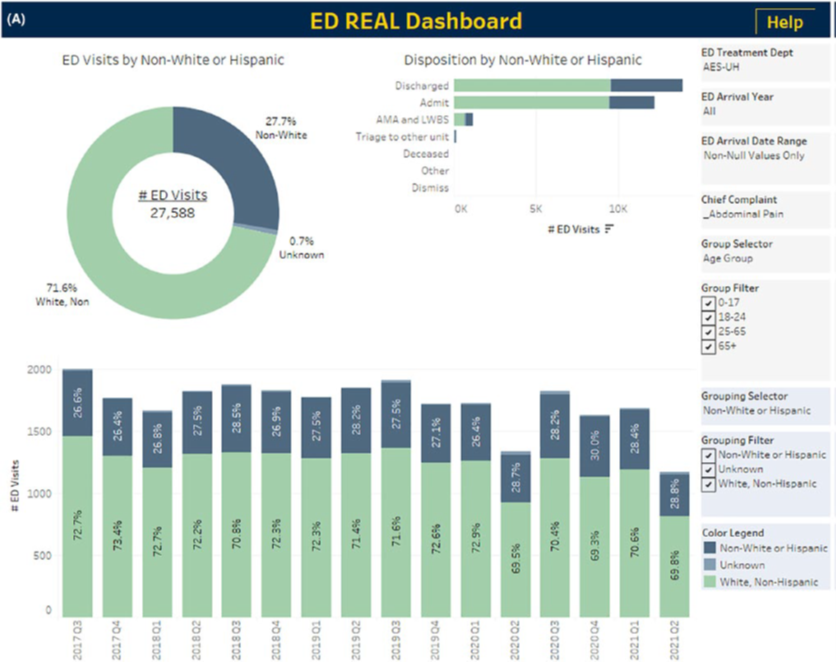
Determine A: Illustration exploratory analyses making use of the dashboard for very first discomfort medication by race and ethnicity in clients presenting with abdominal pain. Actual, Race, Ethnicity, and Language. All panels are filtered to grownup ED visits for stomach pain and stratified by the next teams: White and non-Hispanic, non-White or Hispanic, and not known race/ethnicity. Other selectable filters are at the ideal of each panel. (A) Whole and quarterly distribution of ED visits by race with disposition. Counts and percentages are shown for every single of complete visits, quarterly visits, and tendencies.



More Stories
Thoughts as of late: on evolving, growing & that tiny voice inside
County Health Officials Report 17% Increase in Tuberculosis Cases
10 Most Nutrient-Rich Foods To Include In Your Diet