

Table of Contents
SOAP notes have become indispensable frameworks guiding clinical documentation across healthcare. This article provides mental health professionals with an in-depth guide on leveraging SOAP notes to enhance patient care through accurate record-keeping.
Gathering Subjective Data Critical in Mental Health
The ‘S’ in SOAP notes stands for subjective data, a critical component in mental health, where nearly 50% of diagnoses are derived from patient-reported symptoms (National Institute of Mental Health).
Building trust and rapport facilitates disclosures, which are integral to assessments and treatment plans. Consider conversation starters and tools like journals, surveys, apps, and scales. Document details using the client’s own words while avoiding assumptions or interpretations.
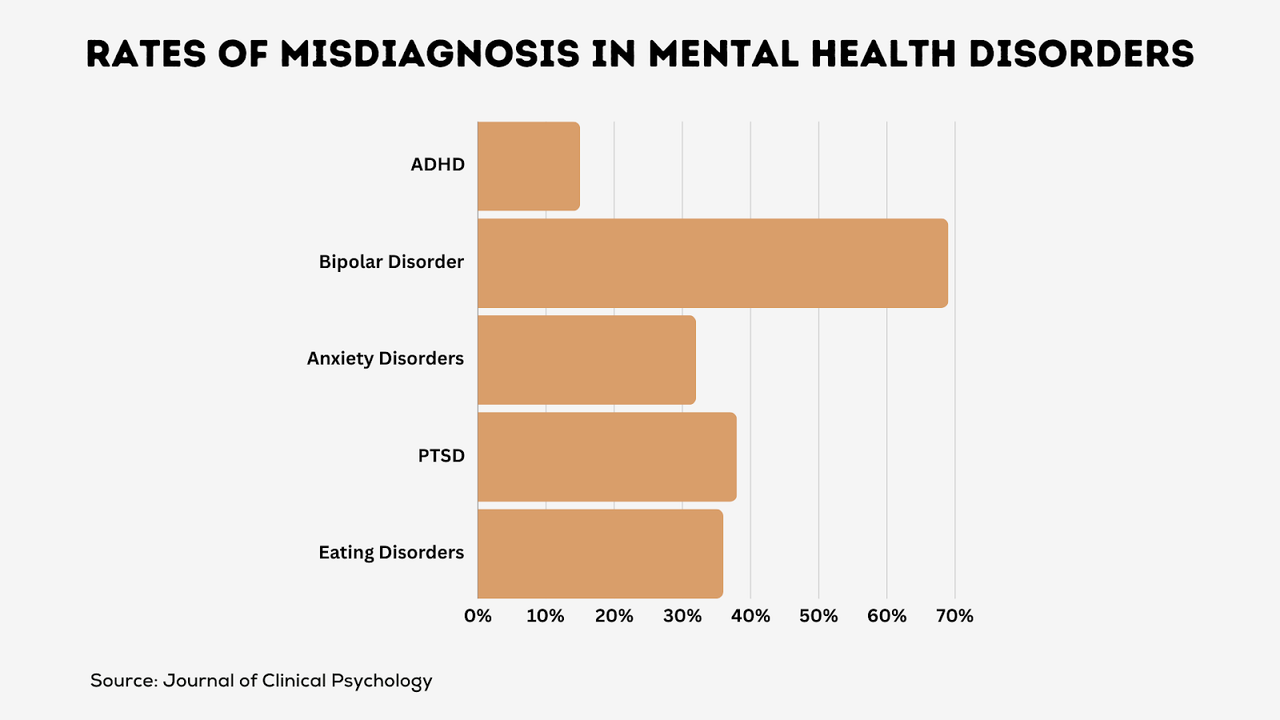
Accurate symptom capture also prevents misdiagnoses carrying risks of inappropriate treatment. For example, symptoms like distraction, common to both anxiety and ADHD, could indicate either condition without sufficient subjective data detailing the patient’s experience. Patient privacy remains paramount when handling sensitive personal information.
> Strong therapeutic alliances and quality subjective data collection associated with better mental health outcomes. (Psychiatric Services)
Infusing Objectivity Into Mental Health Documentation
The “O” section records objective observations including:
- Appearance, orientation, mood, affect, speech patterns, thought processes
- Findings from diagnostic tests, structured interviews, validated rating scales
- Behavioral changes over time based on longitudinal data
Standardized tools like PHQ-9 depression scales, anxiety inventories, suicide risk assessments, and trauma checklists help quantify symptoms.
> Objective metrics establish baselines for tracking mental health progress. (Psychological Assessment)
These tools also help counteract subjective biases that could influence assessments. Formal diagnoses should align with DSM criteria, incorporating structured evaluations that reveal levels of functionality.
Making Informed Assessments in Mental Health Settings
Next, the “A” documents insights into diagnoses, underlying mechanisms, and readiness for change. Assessments integrate:
- Client background, medical history, and prior records
- Diagnoses differentials – rule out possibilities
- Bio-psycho-social formulations identifying causal and maintaining factors
For example, anxiety related to the recent loss of a job and marital issues may link biology (genetic predisposition) with circumstantial stressors and protective factors like social support.
> Accurate diagnosis is essential – misalignment often leads to poor mental health outcomes. (World Psychiatry)
Crafting Personalized Care Plans in Mental Health
The ‘P’ in SOAP notes refers to treatment plans that address areas in need of intervention. Good plans define:
- Goals – What should improve? Desired outcomes?
- Objectives – Incremental steps toward goals
- Interventions – Therapies, techniques, and programs to deploy
- Progress metrics – Symptom rating scales, surveys, behavioral analyses
- Follow-ups – Plan adjusts based on measurable change
Collaborative goal-setting that respects client priorities is vital. For example, a depressed young adult may wish to:
- Goal: Resume college in 6 months
- Objective: Attend 3 classes next semester while raising mood rating from PHQ-9 score of 15 to below 10
- Interventions: Cognitive behavioral therapy, anti-depressant medication, monthly provider follow-ups
- Metrics: PHQ-9 scale, semester course load tracking
Best Practices for Mental Health Documentation
Mental health workers document their patients’ progress using SOAP notes. For those new to this practice, looking into SOAP Note examples can significantly enhance the effectiveness of recording essential information. Given the personal and private nature of these notes, healthcare workers must exercise utmost care to ensure they are written accurately and helpfully. Here are 5 tips:
1. Write a Detailed Personal Story
Share the full picture from sessions without guessing causes. Simply state what you see and hear. For example:
- Todd looked tired with baggy eyes
- Alicia cried for 15 minutes talking about her mom
- Jose said he feels worried at school
Every little detail matters when trying to help.
2. Keep notes private and secure
Health information is private! Follow all ethics rules on:
- Locking up notes
- Needing patient consent to share
- Using online tools safely
Explain to patients how you protect their privacy. Also share if others sometimes may see notes, like if a doctor consults. Assure patients they can opt out.
3. Organize notes carefully
Structure helps! Group-related note parts. List symptoms together. Use lines or headings. Write session highlights at the top. Put them in time order. This makes long notes easier to scan later.
4. Write notes ASAP
Details fade fast! Jot session notes down along the way or right after while it’s fresh. This ensures you capture and share key bits best.
5. Review with patients
Clarify with patients that notes aim to help. Check at the end of sessions:
- Did I miss or misunderstand anything?
- Do you see the progress we’re making?
- What next step seems smartest?
Partnership leads to better care!
Remember, careful progress notes guide better mental health care. Train hard in writing helpful SOAP notes.SMALL daily gains make BIG changes over time!
Integrating SOAP Notes into Mental Health Practice
SOAP notes significantly enhance the delivery of mental health services by:
- Promoting continuity and coordinated care plans across multidisciplinary teams
- Allowing measurement of intervention effectiveness per progress ratings
- Capturing comprehensive data trails on the diagnostic and treatment trajectories
- Generating customizable status summaries for client communication
- Protecting legal interests in case of lawsuits through detailed documentation
Frequently Asked Questions
What ethics or rules should healthcare workers follow with progress notes?
Before starting notes, obtain the patient’s consent and clearly explain how their personal information might be shared. Make sure patients can opt out of certain things whenever they want.
How can SOAP notes assist different healthcare workers in collaborating to support the patient?
SOAP notes follow the same structure across all specialties. So they make it easier for doctors, counselors, nurses, and others to understand a patient’s situation when working together or handing off care.
What are some computer programs that assist with creating and managing progress notes?
Yes! Smart digital tools can make SOAP notes easier and faster to put together, share with other care providers, analyze to find trends, and improve over time. Some popular options used today are SimplePractice, DrChrono, and NextGen.
Bottom Line
In short, careful SOAP note-taking leads to better mental health diagnoses, smarter next steps, and care that puts the patient first. It also lets more healthcare workers collaborate to support that patient.
While learning to write effective progress notes takes practice, the effort is worthwhile. Small gains today bring big wins for care in the future. Additionally, digital tools are available to simplify and enhance this process.



More Stories
Punching Through History: A Spotlight on Boxing Culture in England’s Reading
The Link Between Vitamin E Intake and Parkinson’s Disease
Tips and Techniques for Moving Past Binge Drinking